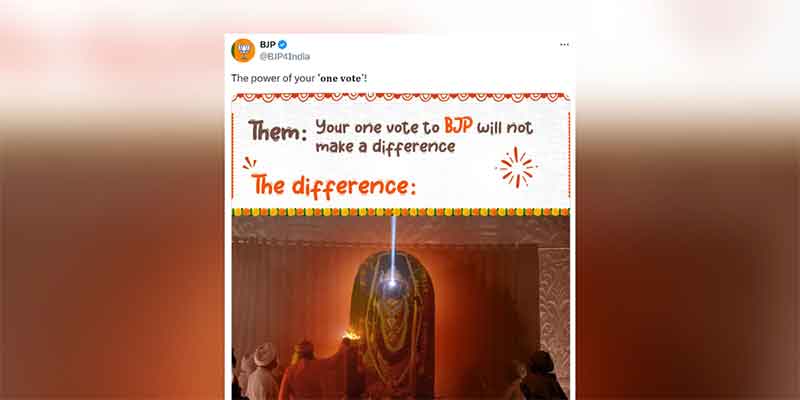
Late last year I started wearing a hijab to protest against the communal virus spread against Muslims by the Indian government by promulgating Citizenship (Amendment) Act, 2019. Now the entire world is facing a secular n-coronavirus which makes no distinction between various religions/ regions/ communities/ class. In India religion wise statistics of infected people is not available and that is exactly how it should be. However, there had been a continuous campaign by the Indian government as well as Delhi government to blame the initial increase in COVID-19 cases once the lockdown was imposed on Tablighi Jamaat. Thus attempting to communalize even a secular n-coronavirus!
Just like the communal virus, n-coronavirus is here to stay with us for quite some time. Long term ways and means to stop the spread of virus at the level of an individual are being devised. These need to become a part of our daily lives just like brushing teeth every day.
To achieve this there is a campaign going on by the Indian government against handshakes and to promote ‘Namaste’ as a greeting; as also to wear facemasks in public. Namaste though widely used now in many Asian countries is a Hindu greeting deriving its roots from Sanskrit and Vedas. Namaste understandably should be a preferred mode of greeting these days as social distancing can be maintained without being rude or disrespectful.
When it comes to facemasks however it will be easy for the Muslim community to adapt to it. Many countries in the past have banned full face-covering hijab worn by Muslim women. Ironically life has come a full circle in these countries as face-covering masks are being promoted all over the world to stop n-coronavirus infection. Centre for Disease Control and Prevention (CDC), Atlanta, U.S.A. has recommended cloth face-covering (e.g. bandana, scarf) to slow the spread of COVID-19.
The adversity humanity is facing could be an opportunity to get rid of the communal virus along with the n-coronavirus. Along with Namaste as a greeting, full face-covering hijab should be promoted as a protection against the virus for both men and women. It is time to universalize hijab and make it gender neutral. It could save the humanity from communal virus, n-coronavirus and who knows may be even patriarchy!
I wear a full face-covering hijab these days whenever I step out of the house.
Shobha Aggarwal is a member of PIL Watch Group and ABVA. Email: [email protected]
SIGN UP FOR COUNTERCURRENTS DAILY NEWS LETTER